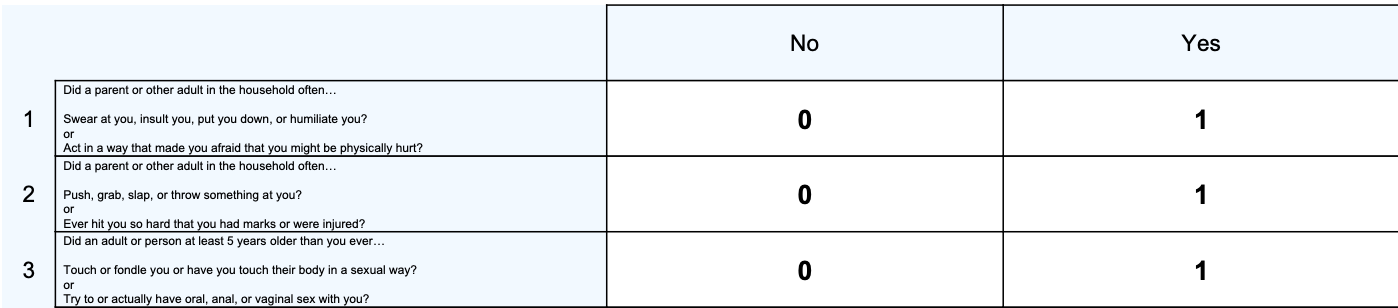

The Adverse Childhood Experiences Questionnaire (ACE-Q) is a 10-item measure to quantify instances of adverse or traumatic experiences that the client has had before the age of 18. The ACE-Q checks for the client’s exposure to childhood psychological, physical, and sexual abuse as well as household dysfunction including domestic violence, substance use, and incarceration.
The ACE-Q can be administered in a self-report manner (for adults or teenagers) or can be reported by parents to indicate the experiences of their child. Given some of the questions may be triggering for trauma clients, some clinicians opt to read the questions to the client and answer the ACE-Q in a collaborative way rather than request self-report.
Clinically, the ACE-Q can be used to help inform treatment because of the connection between adverse childhood experiences, social issues, and adult mental and physical health. The ACE-Q can also help those who have a high score become more informed about their increased risk factor for health issues as well as validate their experiences. People with high scores are likely to benefit from interventions that support their mental health and promote the development of adaptive behaviours.
The ACE-Q was used in the Adverse Childhood Experiences (ACE) Study (Felitti et al., 1998), which found that the ACE-Q score is correlated with later life mental health challenges as well as health risk behaviours (including substance abuse) and serious health problems. These include increased risk for depression, suicide attempts, alcoholism, drug abuse, smoking, 50 or more sexual partners, physical inactivity, severe obesity, sexually transmitted disease, increased risk for broken bones, heart disease, lung disease, liver disease, and multiple types of cancer (Felitti et al., 1998).
A response of Yes for each question is summed to provide an overall ACE-Q score (out of 10). The higher the score, the more adverse childhood experiences the client has had and the higher the risk for social, mental, or other wellbeing problems. The majority of all adults (52%–75%) score one or higher on the ACE-Q (CDC, 2010; Edwards et al., 2007; Ford et al., 2011; Ramiro et al., 2010; Rothman, Bernstein, & Strunin, 2010).
Scores of 4 or more are considered clinically significant. A minority (5%–10%) of the general population score 4 or more, where the general long-term health consequences become most pronounced (Hughes et al., 2017).
Compared with people who have an ACE-Q score of 0, people with an ACE-Q score of 4 are twice as likely to be smokers, 5 times more likely to have depression, 7 times more likely to be alcoholic, 10 times more likely to take illicit drugs, and 12 times more likely to attempt suicide.
Psychometric PropertiesThe ACE Study was completed on over 9,500 individual adults ranging in age from 19 to 92 years of age (Felitti et al., 1998). The ACE Study found that the higher someone’s ACE-Q score – the more types of childhood adversity a person experienced – the higher their risk of chronic disease, mental illness, violence, being a victim of violence and several other consequences.
A graded dose-response association has been found between ACE-Q score and risk for depression, risk for PTSD, relationship problems, emotional distress, worker performance, financial problems, current family problems, high stress, and inability to control anger (Anda et al., 2004; Hillis et al., 2004; Nurius, Logan-Greene, & Green, 2012; Ramiro et al., 2010). High ACE-Q scores also predict risk for homelessness which is especially prevalent in individuals with comorbid substance use disorders and mental illness (Patterson, Moniruzzaman, & Somers, 2014). Findings also suggest that people cannot merely “age out” of the mental health effects of ACEs; adults over the age of 65 with higher ACEs have increased odds of mood and personality disorders (Raposo, Mackenzie, Henriksen, & Afifi, 2014). Compared to people with an ACE-Q score of 0, people with an ACE-Q score of 6 are more likely to have a shorter lifespan by 20 years.
Professional Access
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Anda, R. F., Fleisher, V. I., Felitti, V. J., Edwards, V. J.,Whitfield, C. L., Dube, S. R., & Williamson, D. F. (2004).Childhood abuse, household dysfunction, and indicators of impaired adult worker performance. The Permanente Journal, 8(1), 30–38.
CDC.(2010). Adverse childhood experiences reported by adults—Five states, 2009. MMWR. Morbidity and Mortality Weekly Report, 59(49), 1609–1613.
Edwards, V. J., Anda, R. F., Gu, D., Dube, S. R., & Felitti, V. J.(2007). Adverse childhood experiences and smoking persistence in adults with smoking-related symptoms and illness. The Permanente Journal, 11(2), 5–13.
Ford, E. S., Anda, R. F., Edwards, V. J., Perry, G. S., Zhao, G.,Li, C., & Croft, J. B. (2011).Adverse childhood experiences and smoking status in five states. Preventive Medicine, 53(3), 188–193. https://doi.org/10.1016/j.ypmed.2011.06.015
Hillis, S. D., Anda, R. F., Dube, S. R., Felitti, V. J.,Marchbanks, P. A., & Marks, J. S. (2004). The association between adverse childhood experiences and adolescent pregnancy, long-term psychosocial con-sequences, and fetal death. Pediatrics, 113(2),320–327.